
Abstract
Respiratory syncytial virus (RSV) remains a leading cause of infant morbidity and mortality, with the highest burden concentrated in low- and middle-income countries (LMICs). Existing preventive options, including long-acting monoclonal antibodies, can be constrained by cost, logistics, and access, leaving many high-risk infants unprotected. This article is a structured narrative review summarizing clinical efficacy, immunological mechanisms, safety and public health implications of maternal RSV immunization for preventing infant RSV lower respiratory tract infection (LRTI), with an explicit implementation focus for LMICs. Evidence was identified through targeted searches of major biomedical databases and prioritized by clinical relevance and policy importance, including phase III efficacy trials, regulatory and technical documents, post-authorization safety signals, and modelling studies evaluating potential impact in LMICs. Across the evidence base, maternal vaccination induces robust RSV-neutralizing IgG responses and efficient transplacental antibody transfer, providing passive protection during the first months of life when RSV risk is highest. In phase III data, maternal RSV vaccination demonstrated high efficacy against severe medically attended RSV LRTI in early infancy (e.g., up to 81.8% within the first 90 days for a licensed maternal RSV vaccine). Modelling studies project substantial global reductions in hospitalizations and deaths, although real-world effectiveness in LMICs will depend on antenatal care coverage, timing feasibility, seasonality, and equity of delivery. Safety findings were generally favorable; nonetheless, continued post-licensure monitoring,particularly for pregnancy and birth outcomes such as preterm birth,remains essential. Maternal RSV immunization is a scalable strategy that can leverage existing antenatal platforms and, if equitably implemented, could meaningfully reduce infant RSV morbidity and mortality, especially in LMIC settings.
Similar content being viewed by others

Introduction
Respiratory syncytial virus (RSV) is a major worldwide public health challenge, particularly impacting children in low- and lower-middle-income countries (LMICs). Studies, such as the RSV GOLD, ICU Network, reveal that nearly 29% of children under two admitted to pediatric intensive care units (PICUs) in ten Gavi-supported LMICs tested positive for RSV, with 5% succumbing to the infection [1,2]. Data from the Pneumonia Etiology Research for Child Health study and the Child Health and Mortality Prevention Surveillance study shows that RSV significantly contributes to both pneumonia and infant mortality, making it a major cause of severe respiratory illness in young children [1]. The Global Burden of Disease study attributes one in every 50 deaths among children under five to RSV [3]. Around 20% of infants develop wheezing related to RSV within their first year, and 2% to 3% need hospitalization for the condition [4,5,6]. Estimates indicate that RSV leads to the hospitalization of over 120,000 infants annually in the United States, with the illness causing more than 200 deaths each year [7,8]. These results accentuate the need for comprehensive RSV surveillance and equitable access to preventive interventions, as 97% of RSV-related deaths occur in LMICs, where healthcare resources and access to advanced treatments remain limited [9]. Maternal immunization is an established public-health strategy (e.g., influenza and pertussis vaccination during pregnancy), demonstrating feasibility of antenatal delivery platforms and the principle of protecting young infants via transplacental IgG–mediated passive immunity. In addition to maternal vaccination, long-acting monoclonal antibodies for infants represent a complementary RSV prevention approach, particularly when antenatal access or optimal gestational timing cannot be achieved. Developing reliable measure of outcome for a variety of target populations and the challenges of clinical trials constitute two of the numerous barriers to the development of successful RSV therapies [10]. RSV is perceived as an extremely restricted and fragmented market, which may deter major pharmaceutical investment and impede regulatory routes intended to expedite the licensing of new pharmaceuticals. At the same time, the substantial public health burden of RSV prevents it from being classified as an orphan or neglected disease [11]. Therapeutic alternatives have remained sparse despite improvements in point-of-care diagnostics, RSV epidemiology, and the discovery of antiviral drug candidates. Rapid diagnostic improvements, while advancing point-of-care testing, risk losing valuable data without significant reporting mechanisms to track community-level infections [12]. Comprehensive knowledge of disease mechanisms and extensive clinical trials of novel treatments are necessary for future advancement. Additionally, RSV’s ability to suppress or evade B cell memory complicates vaccine development, raising questions about the feasibility of creating vaccines that elicit durable immunity [13,14]. Enhancing antiviral activity and lowering the likelihood of resistance development may also require combining inhibitors with various modes of action. These issues underscore the need for continued innovation and well-designed clinical trials to address the gaps in RSV prophylactic and therapeutic interventions.
Palivizumab (Synagis) is a monoclonal antibody developed to prevent severe RSV infection. It provides protection against both the A and B virus subtypes by targeting the RSV F-protein, which hinders the virus from fusing with host cells and preventing cell to cell spread [15]. Palivizumab, like all currently available passive or active immunization strategies, does not confer sterilizing immunity and does not completely prevent RSV infection; rather, its benefit lies in reducing disease severity and hospitalization risk [16]. Factors such as insufficient serum concentrations and delays in the injection schedule contribute to these shortcomings. Additionally, adherence to the injection regimen is often challenging, with compliance issues exacerbated by the lack of parental education and logistical barriers [17]. Despite improved compliance through home-based administration, this approach remains costly and difficult to implement on a wide scale [18]. Additionally, palivizumab’s application is limited as it lacks a license to treat established RSV disease [19]. Its potential for reducing the worldwide burden of RSV is hindered by its steep cost, which prevents it from being accessible in resource-poor nations where the bulk of RSV-related deaths occur [18]., however, have evolved substantially beyond palivizumab. Newer long-acting monoclonal antibodies (mAbs), such as nirsevimab and clesrovimab, have been engineered with extended half-lives, allowing protection with a single dose per RSV season [108, 109]. These agents have demonstrated high efficacy in preventing medically attended RSV lower respiratory tract infection and RSV-associated hospitalization in both term and preterm infants. Unlike maternal immunization, long-acting mAbs provide direct, immediate protection to the infant and do not rely on placental antibody transfer or maternal vaccine timing. As such, they are particularly well suited for infants born very preterm, infants with medical comorbidities, and those who may not optimally benefit from maternal immunization due to impaired transplacental antibody transfer or birth outside the optimal vaccination window. Maternal immunization serves a fundamental role in preventing disease in infants, and its use is not a novel concept. Vaccinations against influenza and pertussis during pregnancy are regularly advised in several nations to protect neonates through the transfer of antibodies [20]. In accordance with the passive antibody transfer principle observed in maternal influenza and pertussis vaccination, maternal RSV immunization is a compelling approach of protecting children at their extremely vulnerable hour, prior to their ability to receive vaccine or generate adequate autologous antibodies. Antibodies are transferred to the fetus through the placenta, with maternal IgG serving as the primary antibody subtype [21]. Maternal RSV vaccines offer important population-level advantages, including integration into existing antenatal care platforms and potential scalability in (low- and middle-income countries) LMICs; however, protection is time-limited by antibody waning and may be reduced in preterm infants or those born long after maternal vaccination. Mathematical modeling suggests that maternal RSV immunization can substantially reduce RSV-related hospitalizations in early infancy, particularly within the first three months of life [22]. The U.S. Food and Drug Administration (FDA) authorized Abrysvo, a groundbreaking novel vaccine designed to combat Respiratory Syncytial Virus (RSV), on August 21, 2023 [23,24]. This approval, which acknowledges Abrysvo as a promising preventative strategy against Lower Respiratory Tract Infections (LRTI) resulting from RSV in newborns throughout the critical phase spanning from birth to first six months of life, represents a significant milestone in maternal and infant health [25]. This advancement offers substantial promise in protecting vulnerable infants from severe complications associated with RSV-related LRTI. Abrysvo is a distinctive injectable bivalent prefusion F (preF) protein–based RSV vaccine designed to be administered as a single dose during late pregnancy, commonly between 32 and 36 weeks’ gestation [26]. Rather than using a live-attenuated or inactivated whole RSV virus, it contains stabilized preF antigens that are engineered to elicit robust RSV-neutralizing antibody responses. Following maternal immunization, vaccine-induced IgG antibodies are actively transported across the placenta—particularly in the third trimester—resulting in higher cord blood antibody concentrations and providing infants with passive protection during the early months of life when RSV-associated lower respiratory tract disease risk is highest [27]. This antigen-focused design, combined with optimized timing for transplacental antibody transfer, supports Abrysvo’s potential to reduce RSV-related morbidity in young infants, while emphasizing the importance of programmatic feasibility and antenatal care access to achieve maximal population impact. This review uniquely integrates maternal RSV vaccination and long-acting monoclonal antibodies within a unified passive immunization framework, critically examining their complementary roles, limitations, and implementation relevance for high-risk infants.
Review methodology
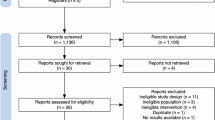
This structured narrative review evaluated the clinical efficacy, immunological mechanisms, safety, and public health implications of maternal RSV immunization, with emphasis on licensed and late-stage maternal vaccine candidates, including Abrysvo. Peer-reviewed literature was searched in PubMed/MEDLINE, Scopus, and Web of Science using Medical Subject Headings (MeSH) and free-text terms such as “Respiratory Syncytial Virus,” “maternal immunization,” “RSV vaccine,” “prefusion F,” “transplacental antibody transfer,” and “lower respiratory tract infection,” combined with Boolean operators (AND/OR). Inclusion criteria comprised English-language publications (2010–2024) reporting original data relevant to maternal RSV vaccination in pregnancy and infant outcomes, including clinical efficacy/effectiveness, immunogenicity and placental antibody transfer, pregnancy and infant safety outcomes, and implementation feasibility. Exclusion criteria included editorials, commentaries, conference abstracts, and secondary reviews without original data, as well as studies not involving pregnant populations or not reporting infant-relevant outcomes. Evidence was prioritized by clinical and policy relevance: (i) phase II/III trials and prespecified infant endpoints (medically attended RSV LRTI, hospitalization, severe disease); (ii) regulatory and technical documents and post-authorization safety monitoring reports to contextualize indications, gestational timing, and safety signals; and (iii) modelling studies, particularly those estimating potential impact in LMICs. Given heterogeneity in study designs, endpoints, and follow-up durations, findings were synthesized descriptively (without meta-analysis). Key clinical, immunological, and public health findings were summarized in tables and figures to enhance transparency and interpretability. The study selection process is summarized in Fig. 1.

Study selection flowchart
Global burden and challenges of RSV in infants: a brief overview
The prevalence of respiratory syncytial virus (RSV)-associated LRTI is highest in low- and middle-income countries (LMICs), and the burden of RSV infection is unequally distributed worldwide (Fig. 2) [1,2]. An estimated 33 million RSV LRTI episodes occurred globally in 2019, leading to 3.6 million hospitalizations and 118,200 fatalities among children younger than five years. Among infants, those under six months of age bear the highest disease burden, accounting for 20% of all RSV infections and nearly 40% of RSV hospitalizations. A more recent 2019 analysis estimated 2.5–4.1 million RSV-related hospitalizations globally. However, most studies on RSV burden have been facility-based, limiting data on community deaths due to challenges in detecting RSV postmortem [28]. Additionally, over half of RSV-related in-hospital deaths occur in infants less than six months. Of these hospitalizations, 61% occur within the first three months of life, emphasizing the vulnerability of this age group to severe disease [29,30,31]. As illustrated in Fig. 1, the global burden of RSV is disproportionately concentrated in low- and middle-income countries, underscoring the urgent need for equitable access to preventive strategies. Further, one-fourth of all RSV LRTI hospitalizations are for preterm infants (born before 37 weeks of gestation), with early preterm infants (born before 32 weeks gestation) having twice the likelihood of needing hospitalization compared to late preterm infants. Approximately 93% of RSV cases, 92% of hospitalizations, and 89% of in-hospital mortality in preterm newborns occur in LMICs, accounting for the majority of these cases [32]. Hospitalizations for RSV LRTI in children under five years old declined substantially in high-income countries (HICs) throughout the COVID-19 pandemic, with hospitalization rates in HICs and upper-middle-income countries falling by about 80% [33]. However, by 2022, rates began to rise again in these regions, although they remained lower in LMICs [34]. This data underscores the significant healthcare disparities between high-income and low-income regions, with the latter facing challenges in providing adequate medical care and access to healthcare services [34,35].

Global Burden of RSV Map. RSV Hospitalization and Mortality Rates. Darker shades indicate higher disease burden, predominantly observed in LMICs
Besides the high disease burden, RSV-associated mortality is particularly severe in LMICs, where over 97% of RSV-related deaths occur [3]. A significant portion of these deaths happen outside of the hospital, often due to a lack of awareness regarding the severity of RSV, with parents in these regions frequently unaware of the risks associated with the infection. RSV was responsible for nearly 41,000 fatalities in children under five and 10.7 million LRTI episodes in 2016 [36]. The total number of RSV-attributable deaths, including those occurring outside the hospital, could be as high as 101,400 [37]. Indeed, insufficient knowledge and delayed medical care may be responsible for up to 20% of RSV-related out-of-hospital mortality in LMICs [29,30,31]. Non-hospitalization rates for severe RSV LRTI are also disproportionately higher in LMICs. For example, studies from South Africa and Kenya has shown that hospitalization rates are comparable in South Africa but three times higher in Kenya for non-hospitalization rates, which occur when children experience severe illnesses but choose not to seek medical care [38,39]. Despite the apparent decrease in RSV hospitalizations in the early pandemic years, the burden of RSV remains substantial in LMICs. It particularly difficult to precisely estimate the number of RSV-related deaths resulting from underreporting, incorrect diagnoses, and considering that many of these deaths take place in community settings rather than hospitals [33]. Even though neonatal deaths from RSV are not as common as those in older children, neonates represent about 20% of RSV-attributable fatalities in the initial six months. This, however, is likely an underestimation due to the nonspecific clinical presentation of RSV in neonates [40]. RSV was identified to be causally linked to 6% of death from pneumonia episodes in Bangladesh and sub-Saharan Africa, according to studies from the Child Health and Mortality Prevention Surveillance (CHAMPS) Network. However, many of these deaths occur in the community, making data collecting a lot more difficult [1,2]. Consequently, RSV death estimates should be viewed as minimal numbers; the true burden may be far greater, especially in LMICs with limited medical services and surveillance. RSV has a substantial influence on critical care services; for instance, a large multicenter study conducted in 2024 found that 30% of children addressed to pediatric intensive care units (PICUs) in LMICs eligible for Gavi had RSV [41]. Despite its significance, limitations such as seasonal sampling, lack of co-infection testing, and disproportionate representation from Nepal (60% of cases) reduce the generalizability of the RSV GOLD—ICU findings [28]. Surveillance initiatives like eSARI provide fundamental data to track RSV seasonality and assess new preventive interventions [42]. Preventive measures like vaccination and better access to healthcare are of paramount importance in communities with limited resources, as preterm newborns are considerably more susceptible for severe illness and hospitalization.
Mechanisms of maternal RSV immunization
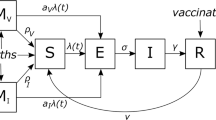
Maternal immunization provides early-life passive protection primarily by inducing RSV-specific neutralizing IgG that is actively transported across the placenta (FcRn-mediated) (Table 1) [43].
Placental IgG transfer increases with gestation and is most efficient in late pregnancy, resulting in high infant antibody levels at birth and protection during early infancy, when RSV risk is greatest [44,45,46]. As illustrated in Fig. 3, maternal RSV vaccination activates innate and adaptive immune pathways that culminate in RSV-specific antibody production and subsequent fetal exposure via transplacental transfer.

Mechanism of antibody-mediated infant protection after maternal RSV vaccination. Maternal RSV vaccination induces innate and adaptive immune responses, promoting placental transfer of RSV-specific IgG to the fetus and resulting in early-life protection against RSV infection. Abbreviations: IgG; immunoglobulin G; RSV; respiratory syncytial virus
As the sole antibody type that can pass through the placenta, IgG protects the fetus against a range of pathogens [47]. The transfer of maternal antibodies offers significant passive protection, particularly in the initial months, before the infant begins receiving vaccinations or generating their own immune responses. The efficiency of placental antibody transfer increases as pregnancy progresses, ensuring that infants are born with a significant level of maternal immunity that helps guard against infections such as influenza, pertussis, and RSV, which can be particularly dangerous during the early stages of life [47]. In addition to placental transfer, breast milk provides an additional layer of immune protection. The primary antibody found in breast milk is IgA, which plays a fundamental role in mucosal immunity, particularly in the gastrointestinal and respiratory tracts. While IgA in breast milk helps provide some ongoing protection against respiratory infections after birth, it is the transplacental IgG that offers more direct and significant immunity to the infant before birth [48]. Additionally, studies reveal that IgG for some pulmonary infections, such COVID-19, can be identified in breast milk, however this is less frequent for other pathogens [47]. As demonstrated by the effectiveness of the influenza and pertussis vaccines, maternal vaccination has long been used to lower the risk of neonatal infections. Considering pertussis, vaccinations in the latter stages of pregnancy (ranging from 27 to 36 weeks gestation) considerably lowers the probability of neonatal pertussis, with up to 95% of neonatal fatalities during their initial few months being successfully prevented [49]. This protective effect is caused by the high quantities of IgG passed through the placenta, which can neutralize the pertussis toxin and offer immunity to the infant till they grow sufficiently mature to acquire their own vaccines [47,50]. A similar strategy is used for RSV immunization. The development of maternal RSV vaccinations attempts to equip infants with passive immunity by triggering the formation of RSV-specific IgG antibodies in the mother, which are then transferred across the placenta [51,52]. Reports have indicated that maternal RSV immunization can considerably lower the rates of RSV-related hospitalizations in newborns, particularly in the initial three months after birth, when maternal IgG levels are at their highest level [22]. An investigation reported a 44% decrease in RSV-related hospitalizations within the initial 90 days following birth utilizing a nanoparticle vaccine called ResVax, composed of the F protein of RSV [53]. However, this protective effect diminishes over time, and by the age of six months, the reduction in hospitalizations becomes minimal, as the infant’s immune system begins to develop its own response and the protective maternal antibodies wane. Mathematical models have demonstrated that maternal RSV immunization could lower hospitalization rates for RSV by as much as 6–37% in neonates younger than three months, with benefits being most prominent in the first few months after birth [22]. These models also show that the benefit of maternal vaccination decreases over time, with a smaller effect observed in children aged three to five months, and minimal impact after six months. Although the findings are promising, the models were based on data from high-income nations, within which hospitalization and fatality rates associated to RSV are lower than in low- and middle-income nations, indicating that regional differences may exist in the advantages of maternal vaccination. Despite the challenges in achieving sustained immunity, the principle of maternal vaccination, utilizing the strategy of transplacental antibody transfer, remains a promising technique for avoiding neonatal and infant morbidity and mortality from RSV and other infectious diseases [54,55]. Ongoing research and clinical trials of RSV vaccines, including those using the pre-F protein to enhance neutralizing antibody responses, hold promise for further improving the protection conferred by maternal immunization [56,57]. One of the critical lessons from earlier experimental RSV vaccine trials, such as those conducted in the 1960s, was the potential risk of enhanced respiratory disease (ERD), primarily mediated by Th2 cells, especially with inactivated RSV vaccines [58,59]. Despite this, maternal immunization with even less effective vaccines, such as formalin-inactivated RSV (FI-RSV), still provided passive protection to offspring, with no significant increase in immunopathology following RSV challenge. This suggests that maternal antibodies can offer substantial protection even when the vaccine itself might pose risks of Th2-mediated immune responses [60,61]. Unlike monoclonal antibodies (mAbs) like palivizumab, which require monthly injections and are limited to high-risk infants, maternal immunization could provide broader coverage without the need for repeated doses [62,63]. Additionally, the infrastructure for maternal vaccines already exists, as seen with influenza and pertussis vaccination programs, potentially enabling smoother implementation. However, challenges remain, including vaccine acceptance among pregnant women, which could affect uptake [46]. While maternal immunization offers indirect protection to the infant, long-acting mAbs provide direct, consistent protection for all infants, lasting at least five months and covering a typical RSV season [64]. Long-acting mAbs can be administered flexibly, offering protection even for infants born outside the RSV season, without relying on the infant’s immune system to mature [65,66,67]. Nevertheless, maternal immunization holds unique advantages, as it not only provides protection for the infant but could potentially offer some benefit to the mother as well, reducing her risk of RSV-associated complications during pregnancy [68, 69]. Both approaches—maternal immunization and long-acting mAbs—play complementary roles in RSV prevention. While mAbs may serve as an effective universal strategy, maternal immunization aligns with existing antenatal care practices, making it a key component in reducing the global RSV burden. Successful implementation will require addressing acceptance barriers, educating stakeholders, and integrating maternal vaccines into routine prenatal care to maximize their impact. Table 1 summarizes key mechanisms of maternal antibody transfer . The overall mechanism of maternal RSV immunization and transplacental antibody transfer is illustrated in Fig. 4 .

Dual Pathways of Infant Protection Induced by Maternal RSV Vaccination. This figure illustrates the immunological mechanisms through which maternal RSV vaccination protects infants both before and after birth. Intramuscular administration of the RSV prefusion F protein vaccine during pregnancy activates maternal antigen-presenting cells (APCs), leading to a CD4⁺ T cell-mediated immune response and the differentiation of plasma cells that produce RSV-specific IgG antibodies. These antibodies cross the placenta, providing passive systemic protection to the fetus, particularly in the lungs. After birth, maternal secretory IgA delivered through breast milk contributes to mucosal immunity in the infant’s respiratory and gastrointestinal tracts. Additionally, monoclonal antibodies may be administered directly to infants as an independent passive protection strategy. Abbreviations: APC, antigen-presenting cell; CD4⁺, cluster of differentiation 4; IgG, immunoglobulin G; IgA, immunoglobulin A; RSV, respiratory syncytial virus
Clinical efficacy of maternal RSV immunization in protecting newborns
Maternal RSV immunization offers a promising strategy to protect newborns by transferring antibodies across the placenta. Several vaccines have been tested for their clinical efficacy in averting severe RSV infections in infants (Table 2, Fig. 5). Comparing the safety and efficacy of various vaccines is fundamental in determining the best effective way to protecting vulnerable newborns.To strengthen cross-platform comparison and reduce repetition, vaccine performance is summarized comparatively across platforms (protein-based preF; nanoparticle; mRNA) and implementation considerations relevant to LMICs are highlighted throughout. Protein-based preF vaccines have the most advanced pregnancy efficacy evidence; nanoparticle vaccines provide supportive but more modest efficacy signals; and mRNA candidates are promising but remain under pregnancy evaluation. In LMICs, expected real-world impact will depend on antenatal coverage, gestational timing feasibility, cold-chain/cost constraints, and local RSV seasonality.
Abrysvo
Abrysvo, approved by the FDA for administration between 32 and 36 weeks of gestation, is administered as a single 0.5 mL intramuscular dose to protect infants from RSV-associated LRTI [70]. The vaccine’s clinical development included rigorous phase 1, phase 2, and phase 3 trials to assess its safety, immunogenicity, and efficacy. Initial phase I/II trials (NCT03529773, registered May 22, 2018) demonstrated significant increases in neutralizing antibody titers, particularly in participants with low baseline immunity. Although decreasing over a year, antibody levels were 4–5 times higher than baseline, indicating immunization in late pregnancy [71]. The trials also confirmed that RSV vaccination did not adversely affect coadministered influenza vaccine responses, although influenza vaccine responsiveness decreased in young adults [72]. A non-inferiority trial assessing the coadministration of RSV and tetanus, diphtheria, and acellular pertussis (Tdap) vaccines was conducted among healthy nonpregnant women in a phase IIb research (NCT04071158). While antibody-induced immunity met non-inferiority criteria for most pathogens, immunogenicity against pertussis was lower compared to single Tdap administration. This underscores the potential of maternal vaccination for multiple pathogens [73]. Another phase IIb trial (NCT04032093) vaccinated pregnant women (24–36 gestational weeks) with two dose formulations, one adjuvanted and one not. Interim 6-month data showed significant maternal antibody production and transfer to infants, significantly reducing infant RSV disease. The unadjuvanted formulation yielded higher infant antibody levels, unaffected by gestational age. Adverse events, including preterm deliveries, were comparable between vaccine and placebo groups, with a 3.7% preterm birth rate overall. The majority of congenital defects were modest and had no correlation with vaccination. Updated data, however, showed that the active group had a greater preterm birth rate (5.3%) than the placebo group (2.6%) [74]. Furthermore, a phase IIa RSV challenge study (NCT04785612) in younger individuals, including not pregnant participants, demonstrated significant protection towards RSV infection [75].
The MATISSE phase III trial (NCT04424316), a randomized, double-blind study, enrolled pregnant women between weeks 24 and 36 of low-risk, uncomplicated pregnancies from 18 countries. This trial demonstrated that Abrysvo significantly decreased the incidence of RSV- linked medically attended severe LRTI in infants. According to interim results, the vaccine efficacy within the first 90 days after birth was 81.8% for severe LRTI. However, the efficacy against RSV-associated LRTI (not severe) was 57.1%, falling short of the statistical success criterion. Protection against severe LRTI within 180 days postpartum was 69.4%. The trial also extensively monitored maternal and infant safety endpoints up to 12 months postpartum. There were no notable safety concerns, and the rate of serious adverse events was comparable across the vaccination and placebo groups. Adverse pregnancy outcomes were comparable, including preeclampsia (1.8% in vaccination recipients vs. 1.4% in placebo) and fetal distress syndrome (1.8% in vaccine vs. 1.4% in placebo). The vaccination group had a slightly greater preterm birth rate (5.7%) than the placebo group (4.7%) [26]. Another phase III trial (NCT05096208) examined the safety and immunogenicity of three distinct vaccination batches, confirming their consistency. The study reaffirmed the favorable safety profile and reactogenicity across vaccine lots [76]. The MORISOT trial (NCT06325657) is a phase III research that recently began to evaluate the efficacy and safety of Abrysvo in pregnant women having stable HIV infection. Eligible participants were in between weeks 24 and 36 of pregnancy. This trial aims to provide data on vaccine performance in immunocompromised populations, extending the applicability of maternal immunization strategies [77,78]. The FDA requires ongoing safety monitoring through systems like the Vaccine Adverse Event Reporting System (VAERS), directed by the CDC and FDA. VAERS data since January 2023 to April 2024 reported 199 serious adverse events, including premature labor (28 cases), cesarean deliveries (8), and preterm premature rupture of membranes (6). Of the premature labor cases, 21 were reported in women aged 30–39 years. Although the VAERS data align with clinical trial findings, such as the incidence of preterm births (5.7% in the vaccine group vs. 4.7% in the placebo group), it lacks the ability to establish definitive causal links due to its reliance on passive reporting. This limitation necessitates careful interpretation and further investigation. Ongoing Phase 4 studies and systematic reviews are essential to confirm the vaccine’s safety, refine its risk profile, and ensure the benefits of preventing RSV-associated illness significantly outweigh any potential risks [26].
RSV MAT
Targeting precisely the same prefusion F protein as Abrysvo, GSK plc’s maternal RSV vaccine candidate, RSV MAT, has undergone several clinical studies. NCT03674177, the first-in-human phase I study, evaluated immunogenicity and safety in non-pregnant women. It showed a favorable safety profile and supported further investigation during pregnancy [79].
In the phase II trial (NCT04126213), pregnant women (28–33 weeks gestation) received the vaccine, showing a comparable safety profile to the placebo group. Adverse events, including preterm labor and congenital anomalies, occurred at similar rates between groups, though a slight increase in hypertension and preeclampsia cases was noted but remained within general population levels. Both vaccinated women and the newborns showed elevated RSV-specific antibody titers [80]. Another phase II trial (NCT04138056) evaluated coadministration with Diphtheria-Tetanus-Pertussis (DTaP) vaccines in non-pregnant women. Although no significant interference in RSV immunogenicity was detected, mild interference was observed in DTaP responses, particularly for pertussis, with unknown clinical implications [81]. A large-scale phase III investigation, the GRACE trial (NCT04605159) assessed the vaccine’s efficacy and safety in preventing infants from developing lower respiratory tract disease (LRTD) caused by RSV. While efficacy was satisfactory, the trial was prematurely halted due to safety concerns, notably a higher preterm birth rate (6.8% in vaccinated vs. 4.9% in placebo groups) [82]. These findings led to the discontinuation of other trials, including NCT04980391 (high-risk pregnancies) and NCT05229068 (re-vaccination trial) [83,84]. A smaller phase III trial (NCT05169905) in non-pregnant females enrolled only nine participants before being terminated. However, another ongoing phase III trial (NCT05045144) continues to assess different vaccine lots and coadministration with influenza vaccines in non-pregnant women. To address safety concerns, GSK initiated a phase IIIb open-label trial (NCT05705440) for long-term follow-up of participants from previous studies [85,86,87]. GSK previously developed another maternal RSV vaccine candidate, GSK3003891A, which was abandoned due to formulation instability. The development of RSV MAT highlights the complexities of balancing efficacy and safety, particularly in vulnerable populations like pregnant women [88].
ResVax
Novavax, Inc. developed ResVax, a nanoparticle vaccine that encodes the RSV F protein. Its clinical development spanned multiple phases. Initiated in 2011, the Phase I Trial (NCT01290419) evaluated the vaccine in young male and female participants. The vaccine demonstrated an acceptable safety profile, with no toxicity observed and a marked increase in RSV-specific antibody titers, supporting progression to phase II trials [89].
Two trials were carried out to enhance the vaccine’s dosage and ascertain the effects of adding an adjuvant (NCT01704365, NCT01960686). There were fewer RSV infections after vaccinations, and enrolled women between the ages of 18 and 35 reported no serious safety issues. These results led to the selection of a mid-level adjuvant dosage in conjunction with a high antigen dose for maternal immunization trials [90,91]. Pregnant women in their third trimester were recruited for another phase II study (NCT02247726), which followed up with the infants for a year. Without raising any safety concerns, the vaccination showed protection against severe RSV infections in both women and infants. A significant amount of newborn antibodies with an average half-life of 40 days were found by cord blood analysis [92]. Participants in the major phase III study (NCT02624947) included pregnant women between weeks 28 and 36 of pregnancy. With similar rates of low birth weight, preterm delivery, and intrauterine growth restriction across the vaccination and placebo groups, no significant safety concerns were observed. The vaccine, however, failed to fulfill the established effectiveness threshold for medically serious lower respiratory tract infections (LRTIs) unique to RSV. Efficacy against RSV LRTI was 39.4% up to 3 months of age, and it increased to 58.8% for severe illness with hypoxemia. Remarkably, comparable effectiveness rates were seen for hospitalizations and all-cause LRTI. Although the study lacked statistical power to assess effectiveness on a country-specific basis, data also indicated greater protection against hospitalizations and severe cases in LMICs [93]. Despite promising data, ResVax is no longer part of Novavax’s development pipeline.
mRNA-1345
Moderna Inc. developed mRNA-1345, an mRNA-based RSV vaccine that targets the RSV F protein and is delivered effectively via lipid nanoparticles. In the NCT04528719 Phase I study, women and other healthy young individuals underwent vaccination. The results demonstrated a favorable safety profile, with elevated RSV-specific antibody titers observed within six months post-vaccination. These promising outcomes supported the vaccine’s potential for maternal immunization [94]. Pregnant women between the ages of 28 and 36 weeks are being recruited for the phase II study (NCT06143046). With follow-up scheduled for both mother participants and their infants, the investigation intends to assess the vaccine’s safety, immunogenicity, and effectiveness [95].
V-306
Virometix AG’s vaccine candidate V-306 targets the RSV F protein’s FsIIm epitope. The vaccine failed to provide the expected neutralizing or IgG-specific immunity in the phase I study (NCT04519073). Consequently, it could be necessary to modify the formulation of V-306 in order to attain the intended immunogenic response [96].

Comparative overview of maternal vaccines under development against respiratory syncytial virus (RSV). This figure illustrates the current status of five maternal vaccine candidates designed for administration during pregnancy to protect newborns against lower respiratory tract infections (LRTIs) caused by RSV. Each area displays the technological platform, regulatory status, available data on clinical efficacy and immunogenicity, relevant safety signals (particularly preterm birth), and the estimated feasibility of implementation in low- and middle-income countries (LMICs). Included are vaccines based on protein subunits (Abrysvo and RSV MAT), nanoparticles (ResVax), mRNA (mRNA-1345), and synthetic peptides (V-306). Color-coded icons indicate key features such as reported efficacy (), development halted due to safety (), lack of clinical data (❔), and visual classification of LMIC viability ( ◍ high, ◍ moderate, ◍ low). The central illustration emphasizes the maternal-fetal focus of this preventive strategy. Information is based on completed or ongoing clinical trials as detailed in the main text
Public health implications and policy considerations for RSV maternal immunization
Broader health implications of RSV maternal immunization
The broader health implications of RSV maternal immunization extend beyond reducing infant mortality. By averting a significant number of RSV-related hospitalizations and deaths, particularly in LMICs, maternal vaccines can alleviate the burden on healthcare systems, reduce economic costs associated with infant care, and improve long-term health outcomes for vulnerable populations [97]. Additionally, the widespread implementation of maternal immunization programs can enhance global health equity by prioritizing regions with limited access to healthcare and high RSV mortality rates. These efforts also highlight the importance of strengthening antenatal care services, ensuring optimal vaccine timing during pregnancy, and addressing barriers such as vaccine accessibility and public awareness. The potential success of RSV maternal immunization serves as a model for other maternal vaccine initiatives, underscoring the critical role of maternal health interventions in achieving broader public health goals [1,2,98].
Across 73 Gavi-supported countries, modeling studies projected that RSV MI could prevent 10 to 12 million RSV cases, 8.5 to 112 million disability-adjusted life years (DALYs), and 123,000 to 177,000 deaths between 2023 and 2035 [99,100]. A 42% reduction in RSV-attributable deaths among infants younger than six months in Gavi countries. Studies conducted in Kenya further indicate that RSV MI could lead to a 32% decrease in RSV infections and a 50% reduction in hospitalizations due to RSV [101,102]. These findings align with projections for other life-saving vaccines, such as the rotavirus vaccine, which averted 36% of rotavirus-related diarrheal deaths among children under five in similar regions. Another modeling study estimated that maternal RSV immunization could significantly reduce the burden of RSV-associated LRTIs among U.S. infants. In the absence of immunization, approximately 590,000 medically attended RSV LRTIs occur annually [103]. Maternal immunization administered year-round is projected to prevent around 74,000 healthcare visits annually, spanning outpatient, emergency department (ED), and hospitalization settings. However, the impact of maternal vaccines may be influenced by their shorter duration of protection, which is assumed to be 90 days. Sensitivity analyses revealed that a 10% increase in maternal vaccine uptake could avert an additional 2,730–16,110 outpatient visits, 820–5,880 ED visits, and 580–2,150 hospitalizations. These findings underscore the potential of maternal immunization to mitigate RSV-related morbidity in early infancy and reduce the associated healthcare burden [22]. The success of maternal RSV immunization serves as a framework for strengthening other maternal vaccine programs. However, gaps in understanding remain, such as differences in vaccine efficacy across income settings, the mechanisms of broader protective effects (e.g., reduced all-cause pneumonia), and logistical challenges in vaccine delivery. Addressing these issues will be vital to maximizing the health benefits of maternal RSV immunization and ensuring equitable access for vulnerable populations [50].
Public health and policy considerations
In 2019, PATH and the WHO released a roadmap to advance maternal RSV immunization (RSV MI), emphasizing the global priority of RSV prevention due to high rates of hospitalizations and deaths, particularly in infants under six months [104]. The roadmap identified gaps in RSV disease data, vaccine efficacy, and health economics, with a focus on supporting LMICs through standardized data collection, funding, and access to WHO-prequalified vaccines. Essential measures include promoting evidence-based decision-making, guaranteeing fair delivery systems, and making sure that vaccinations are accessible, safe, and reasonably priced.
Post-phase III clinical trial data, such as from Novavax, show reduced RSV-related hospitalizations but did not meet primary endpoints. Ongoing clinical questions, such as vaccine efficacy variations between high- and low-income countries, need further exploration. As more data emerge, preparations should focus on raising awareness, enhancing collaboration between immunization and maternal health programs, improving operational readiness, and monitoring local RSV epidemiology and vaccine safety [53]. Despite the inconclusive trial results, maternal immunization offers significant health benefits. Policymakers ought to keep pushing for its inclusion in international health plans, filling up information gaps, and bolstering the use of vaccines in RSV-affected nations. When a maternal RSV vaccination becomes accessible, its application in many contexts depends on further research and operational initiatives. Educating stakeholders about RSV infections and the advantages of maternal vaccination is part of this. Maternal, Neonatal, and Child Health (MNCH) programs, which are frequently in charge of administering vaccines, and Expanded Programs on Immunization (EPI) must collaborate more effectively. Additionally, establishing significant operations and logistics for vaccine procurement, distribution, and monitoring is fundamental, as is setting up systems to track local epidemiology and assess vaccine safety and impact [105,106,107].
Future directions and clinical gaps
In LMICs, where RSV continues to be a major cause for infant morbidity and mortality, maternal RSV vaccination has the potential to significantly reduce the virus’s impact. However, clinical and operational challenges persist. While phase III trials have shown benefits like reduced hospitalizations, questions remain about the mechanisms of protection, especially regarding severe RSV-related pneumonia and hypoxemia. The variability in vaccine efficacy between high- and low-income settings needs further investigation, particularly for preterm infants, who are at higher risk for severe infections. Operationally, the success of maternal RSV immunization in LMICs depends on ensuring safe, effective, and affordable vaccines, strengthening health systems, and improving coordination between maternal health and immunization programs. It’s also essential to develop infrastructure to monitor the epidemiology, safety, and impact of the vaccine once implemented. Future efforts should focus on addressing these gaps, particularly improving vaccine formulations and understanding how vaccines perform across diverse populations. Continued surveillance, real-world data collection, and strengthening immunization systems will be fundamental for the widespread success of maternal RSV vaccination [53].
Conclusions
In conclusion, maternal RSV immunization represents a critical advancement in the prevention of RSV- associated morbidity and mortality, predominantly in high-risk populations like preterm infants, infants under six months, and those residing in low- and middle-income countries (LMICs). The results from clinical trials and modeling studies suggests that vaccinating pregnant women could considerably decrease the global RSV burden by preventing severe infections in infants and minimizing hospitalizations, particularly in regions with limited access to healthcare. By targeting pregnant women, maternal immunization offers an effective strategy to provide passive immunity to infants who are most vulnerable during their early months of life. Furthermore, the positive outcomes from maternal RSV immunization trials could pave the way for similar vaccine strategies in preventing other respiratory infections, such as influenza and pertussis, thereby strengthening maternal immunization programs worldwide. This approach could lead to substantial improvements in public health outcomes, enhancing healthcare access and equity, especially in LMICs where the burden of RSV is highest. Finally, integrating maternal RSV immunization into global health policies could play a pivotal role in reducing the disproportionate mortality and healthcare costs associated with RSV, making it a key intervention in achieving broader health equity and improving overall maternal and child health.
Data availability
Not Applicable.
Abbreviations
- APCs:
-
Antigen presenting cells
- BCR:
-
B cell receptor
- CD4:
-
Cluster of differentiation 4
- CDC:
-
Centers for Disease Control and Prevention
- DALYs:
-
Disability-adjusted life years
- DTaP:
-
Diphtheria-tetanus-acellular pertussis
- ED:
-
Emergency department
- EPI:
-
Expanded Program on Immunization
- ERD:
-
Enhanced respiratory disease
- FDA:
-
Food and Drug Administration
- FI-RSV:
-
Formalin-inactivated respiratory syncytial virus
- GA:
-
Gestational age
- GI:
-
Gastrointestinal
- GSK:
-
GlaxoSmithKline
- HICs:
-
High-income countries
- HIV:
-
Human immunodeficiency virus
- ICU:
-
Intensive care unit
- IgA:
-
Immunoglobulin A
- IgG:
-
Immunoglobulin G
- LMICs:
-
Low- and middle-income countries
- LRTD:
-
Lower respiratory tract disease
- LRTI:
-
Lower respiratory tract infection
- mAbs:
-
Monoclonal antibodies
- MI:
-
Maternal immunization
- MNCH:
-
Maternal, Neonatal, and Child Health
- MHC:
-
Major histocompatibility complex
- PATH:
-
Program for Appropriate Technology in Health
- PICU:
-
Pediatric intensive care unit
- RSV:
-
Respiratory syncytial virus
- Tdap:
-
Tetanus-diphtheria-acellular pertussis
- TCR:
-
T cell receptor
- VAERS:
-
Vaccine Adverse Event Reporting System
- WHO:
-
World Health Organization
References
O’Brien KL, et al. Causes of severe pneumonia requiring hospital admission in children without HIV infection from Africa and asia: the PERCH multi-country case-control study. Lancet. Aug. 2019;394(10200):757–79. https://doi.org/10.1016/S0140-6736(19)30721-4.
Blau DM et al. Sep., Deaths Attributed to Respiratory Syncytial Virus in Young Children in High–Mortality Rate Settings: Report from Child Health and Mortality Prevention Surveillance (CHAMPS), Clinical Infectious Diseases, vol. 73, no. Supplement_3, pp. S218–S228, 2021, https://doi.org/10.1093/cid/ciab509
Li Y, et al. Global, regional, and National disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet. May 2022;399(10340):2047–64. https://doi.org/10.1016/S0140-6736(22)00478-0.
Boyce TG, Mellen BG, Mitchel EF, Wright PF, Griffin MR. Rates of hospitalization for respiratory syncytial virus infection among children in Medicaid, J Pediatr, vol. 137, no. 6, pp. 865–870, Dec. 2000, https://doi.org/10.1067/mpd.2000.110531
KIM HW, EPIDEMIOLOGY, OF RESPIRATORY SYNCYTIAL VIRUS INFECTION IN WASHINGTON DC et al. Am J Epidemiol, vol. 98, no. 3, pp. 216–225, Sep. 1973, https://doi.org/10.1093/oxfordjournals.aje.a121550
Glezen WP. Risk of primary infection and reinfection with respiratory syncytial virus. Arch Pediatr Adolesc Med. Jun. 1986;140(6):543. https://doi.org/10.1001/archpedi.1986.02140200053026.
Shay DK, Holman RC, Roosevelt GE, Clarke MJ, Anderson LJ. Bronchiolitis-Associated Mortality and Estimates of Respiratory Syncytial Virus–Associated Deaths among US Children, 1979–1997, J Infect Dis, vol. 183, no. 1, pp. 16–22, Jan. 2001, https://doi.org/10.1086/317655
Shay DK, Among B-AH, Children US. 1980–1996, JAMA, vol. 282, no. 15, p. 1440, Oct. 1999. https://doi.org/10.1001/jama.282.15.1440
MacNeil, McMorrow M. RSV burden and prevention in children in LMICs. Oct 01. 2024. https://doi.org/10.1016/S2214-109X(24)00289-4. Elsevier Ltd.
Simoes EAF, et al. Challenges and opportunities in developing respiratory syncytial virus therapeutics. J Infect Dis. Mar. 2015;211(1):S1–20. https://doi.org/10.1093/infdis/jiu828.
Kumar N, Kumar RN, Patil N, Soni H. Studies on plant species used by tribal communities of Saputara and Purna forests, Dangs district. Gujarat; 2007.
HENRICKSON KJ. Advances in the laboratory diagnosis of viral respiratory disease. Pediatr Infect Disease J. Jan. 2004;23(1):S6–10. https://doi.org/10.1097/01.inf.0000108187.63151.ea.
Griffiths C, Drews SJ, Marchant DJ. Respiratory syncytial virus: Infection, Detection, and new options for prevention and treatment. Clin Microbiol Rev. Jan. 2017;30(1):277–319. https://doi.org/10.1128/CMR.00010-16.
Habibi MS, et al. Impaired Antibody-mediated protection and defective IgA B-Cell memory in experimental infection of adults with respiratory syncytial virus. Am J Respir Crit Care Med. May 2015;191(9):1040–9. https://doi.org/10.1164/rccm.201412-2256OC.
YOUNG J. Development of a potent respiratory syncytial virus-specific monoclonal antibody for the prevention of serious lower respiratory tract disease in infants. Respir Med. Apr. 2002;96:S31–5. https://doi.org/10.1053/rmed.2002.1298.
Palivizumab prophylaxis of respiratory syncytial virus disease. In 2000–2001: results from the Palivizumab outcomes registry. Pediatr Pulmonol. Jun. 2003;35(6):484–9. https://doi.org/10.1002/ppul.10288.
Fenton C, Scott LJ, Plosker GL. Palivizumab: A review of its use as prophylaxis for serious respiratory syncytial virus infection. Pediatr Drugs. 2004;6(3):177–97. https://doi.org/10.2165/00148581-200406030-00004.
Golombek SG, Berning F, Lagamma EF. Compliance with prophylaxis for respiratory syncytial virus infection in a home setting., Pediatr Infect Dis J, vol. 23, no. 4, pp. 318–22, Apr. 2004, https://doi.org/10.1097/00006454-200404000-00008
Rogovik L, Carleton B, Solimano A, Goldman RD. Palivizumab for the prevention of respiratory syncytial virus infection., Can Fam Physician, vol. 56, no. 8, pp. 769–72, Aug. 2010.
V. Romanin et al., Maternal Vaccination in Argentina: Tetanus, Diphtheria, and Acellular Pertussis Vaccine Effectiveness During Pregnancy in Preventing Pertussis in Infants <2 Months of Age, Clinical Infectious Diseases, vol. 70, no. 3, pp. 380–387, Jan. 2020, doi: 10.1093/cid/ciz217.
Ciobanu M, Dumitru AE, Gica N, Botezatu R, Peltecu G, Panaitescu AM. Benefits and risks of IgG transplacental transfer. Diagnostics. Aug. 2020;10(8):583. https://doi.org/10.3390/diagnostics10080583.
Hogan B, et al. Potential impact of a maternal vaccine for RSV: A mathematical modelling study. Vaccine. Oct. 2017;35(45):6172–9. https://doi.org/10.1016/j.vaccine.2017.09.043.
Halsey G, Pfizer Wins FDA Approval for Vaccine against RSV in Older Adults, Care P, Online.), p. NA, 2023. [Online]. Available: https://link.gale.com/apps/doc/A777403118/AONE?u=anon~9f968d9d&sid=googleScholar&xid=8800b4a8
FDA Approves First Vaccine for Pregnant Individuals to Prevent RSV. in Infants | FDA. Accessed: Dec. 30, 2024. [Online]. Available: https://www.fda.gov/news-events/press-announcements/fda-approves-first-vaccine-pregnant-individuals-prevent-rsv-infants
Amin R, Dhama K, Emran TB. Influenza and respiratory syncytial virus interbreed: engendering a novel deadly virus. Int J Surg. Feb. 2023;109(2):184–5. https://doi.org/10.1097/JS9.0000000000000187.
Kampmann et al. Apr., Bivalent Prefusion F Vaccine in Pregnancy to Prevent RSV Illness in Infants, New England Journal of Medicine, vol. 388, no. 16, pp. 1451–1464, 2023, https://doi.org/10.1056/NEJMoa2216480
Patel J, Chawla, Blavo C. Use of the Abrysvo vaccine in pregnancy to prevent respiratory syncytial virus in infants: A review. Cureus Aug. 2024. https://doi.org/10.7759/cureus.68349.
Li Y, et al. National burden estimates of hospitalisations for acute lower respiratory infections due to respiratory syncytial virus in young children in 2019 among 58 countries: a modelling study. Lancet Respir Med. Feb. 2021;9(2):175–85. https://doi.org/10.1016/S2213-2600(20)30322-2.
Koffi K, Maina A, Yaroh AG, Habi O, Bensaïd, and, Kalter HD. Social determinants of child mortality in niger: results from the 2012 National verbal and social autopsy study. J Glob Health. 2016;6(1):010603. https://doi.org/10.7189/JOGH.06.010603.
Mazur NI, Caballero MT, Nunes MC. Respiratory syncytial virus 2024 1 severe respiratory syncytial virus infection in children: burden, management, and emerging therapies. Lancet. 2024;404:1143–56. https://doi.org/10.1016/S0140-6736(24)01716-1.
Caballero MT, et al. Mortality associated with acute respiratory infections among children at home. J Infect Dis. Jan. 2019;219(3):358–64. https://doi.org/10.1093/INFDIS/JIY517.
Wang X et al. Mar., Global disease burden of and risk factors for acute lower respiratory infections caused by respiratory syncytial virus in preterm infants and young children in 2019: a systematic review and meta-analysis of aggregated and individual participant data, Lancet, vol. 403, no. 10433, pp. 1241–1253, 2024, https://doi.org/10.1016/S0140-6736(24)00138-7
Chow J, Uyeki TM, Chu HY. The effects of the COVID-19 pandemic on community respiratory virus activity, Nat Rev Microbiol, vol. 21, no. 3, pp. 195–210, Mar. 2023, https://doi.org/10.1038/S41579-022-00807-9
Cong B, et al. Changes in the global hospitalisation burden of respiratory syncytial virus in young children during the COVID-19 pandemic: a systematic analysis. Lancet Infect Dis. Apr. 2024;24(4):361–74. https://doi.org/10.1016/S1473-3099(23)00630-8.
Izu et al. Sep., All-cause and pathogen-specific lower respiratory tract infection hospital admissions in children younger than 5 years during the COVID-19 pandemic (2020-22) compared with the pre-pandemic period (2015-19) in South Africa: an observational study, Lancet Infect Dis, vol. 23, no. 9, pp. 1031–1041, 2023, https://doi.org/10.1016/S1473-3099(23)00200-1
Troeger, et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–. Lancet Infect Dis. Nov. 2018;18(11):1191–210. https://doi.org/10.1016/S1473-3099(18)30310-4. 2016: a systematic analysis for the Global Burden of Disease Study 2016.
Shi T, et al. Global, regional, and National disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: a systematic review and modelling study. Lancet. Sep. 2017;390(10098):946–58. https://doi.org/10.1016/S0140-6736(17)30938-8.
Moyes J et al. Dec., The burden of RSV-associated illness in children aged < 5 years, South Africa, 2011 to 2016, BMC Med, vol. 21, no. 1, pp. 1–10, 2023, https://doi.org/10.1186/S12916-023-02853-3/FIGURES/3
Nyawanda BO, et al. Estimates of the National burden of respiratory syncytial virus in Kenyan children aged under 5 years, 2010–2018. BMC Med. Dec. 2023;21(1). https://doi.org/10.1186/S12916-023-02787-W.
Gill CJ, et al. Infant deaths from respiratory syncytial virus in Lusaka, Zambia from the ZPRIME study: a 3-year, systematic, post-mortem surveillance project. Lancet Glob Health. Feb. 2022;10(2):e269–77. https://doi.org/10.1016/S2214-109X(21)00518-0.
Abdelrahman N, et al. Respiratory syncytial virus infection among children younger than 2 years admitted to a paediatric intensive care unit with extended severe acute respiratory infection in ten Gavi-eligible countries: the RSV GOLD—ICU network study. Lancet Glob Health. Oct. 2024;12(10):e1611–9. https://doi.org/10.1016/S2214-109X(24)00269-9.
Summary report on the WHO workshop on estimation of respiratory syncytial. virus (RSV) disease burden based on RSV surveillance of Global Influenza Surveillance and Response System, Geneva, Switzerland, 21–23 June 2023. Accessed: Jan. 03, 2025. [Online]. Available: https://www.who.int/publications/i/item/9789240092846
Malek R, Sager P, Kuhn KH, Nicolaides, Schneider H. Evolution of maternofetal transport of Immunoglobulins during human pregnancy. Am J Reprod Immunol. Nov. 1996;36(5):248–55. https://doi.org/10.1111/J.1600-0897.1996.TB00172.X.
Etti M, et al. Maternal vaccination: a review of current evidence and recommendations. Am J Obstet Gynecol. Apr. 2022;226(4):459–74. https://doi.org/10.1016/J.AJOG.2021.10.041/ATTACHMENT/E3183BC9-E2D4-450D-AAD7-E6F7D56101B1/MMC2.MP4.
Child. and Adolescent Immunization Schedule by Age | Vaccines & Immunizations | CDC. Accessed: Jan. 06, 2025. [Online]. Available: https://www.cdc.gov/vaccines/hcp/imz-schedules/child-adolescent-age.html?CDC_AAref_Val=https://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html
Esposito S, et al. RSV prevention in all infants: which is the most preferable strategy? Front Immunol. Apr. 2022;13:880368. https://doi.org/10.3389/FIMMU.2022.880368/BIBTEX.
Ogilvie MM, Santhire Vathenen A, Radford M, Codd J, Key S. Maternal antibody and respiratory syncytial virus infection in infancy, J Med Virol, vol. 7, no. 4, pp. 263–271, Jan. 1981, https://doi.org/10.1002/JMV.1890070403
Murray, Chu HY. RSV, Antibodies and the Developing World, Pediatric Infectious Disease Journal, vol. 38, no. 6, p. S24, Jun. 2019, https://doi.org/10.1097/INF.0000000000002333
Amirthalingam D et al. 2016, https://doi.org/10.1093/CID/CIW559
Gunatilaka, Giles ML. Maternal RSV vaccine development. Where to from here? Hum Vaccin Immunother. 2021;17(11):4542–8. https://doi.org/10.1080/21645515.2021.1955608.
Glezen WP, Paredes A, Allison JE, Taber LH, Frank AL. Risk of respiratory syncytial virus infection for infants from low-income families in relationship to age, sex, ethnic group, and maternal antibody level. J Pediatr. May 1981;98(5):708–15. https://doi.org/10.1016/S0022-3476(81)80829-3.
Stensballe LG, et al. Respiratory syncytial virus neutralizing antibodies in cord blood, respiratory syncytial virus hospitalization, and recurrent wheeze. J Allergy Clin Immunol. Feb. 2009;123(2):398–403. https://doi.org/10.1016/j.jaci.2008.10.043.
Madhi SA et al. Jul., Respiratory Syncytial Virus Vaccination during Pregnancy and Effects in Infants, New England Journal of Medicine, vol. 383, no. 5, pp. 426–439, 2020,
Chu Y et al. Nov., Respiratory syncytial virus transplacental antibody transfer and kinetics in mother-infant pairs in Bangladesh, J Infect Dis, vol. 210, no. 10, pp. 1582–1589, 2014, https://doi.org/10.1093/INFDIS/JIU316
Glezen WP, Paredes A, Allison JE, Taber LH, Frank AL. Risk of respiratory syncytial virus infection for infants from low-income families in relationship to age, sex, ethnic group, and maternal antibody level. J Pediatr. 1981;98(5):708–15. https://doi.org/10.1016/S0022-3476(81)80829-3.
Eichinger KM, Kosanovich JL, Lipp M, Empey KM, Petrovsky N. Strategies for active and passive pediatric RSV immunization. Ther Adv Vaccines Immunother. Feb. 2021;9. https://doi.org/10.1177/2515135520981516/ASSET/IMAGES/LARGE/10.1177_2515135520981516-FIG3.JPEG.
Capella F, Postfusion F, Antibodies G et al. and Disease Severity in Infants and Young Children With Acute Respiratory Syncytial Virus Infection, J Infect Dis, vol. 216, no. 11, pp. 1398–1406, Dec. 2017, https://doi.org/10.1093/INFDIS/JIX489
Knudson J, Hartwig SM, Meyerholz DK, Varga SM. RSV Vaccine-Enhanced Disease Is Orchestrated by the Combined Actions of Distinct CD4 T Cell Subsets, PLoS Pathog, vol. 11, no. 3, p. e1004757, Mar. 2015, https://doi.org/10.1371/JOURNAL.PPAT.1004757
Castilow M, Meyerholz DK, Varga SM. IL-13 is required for eosinophil entry into the lung during respiratory syncytial virus vaccine-enhanced disease, J Immunol, vol. 180, no. 4, pp. 2376–2384, Feb. 2008, https://doi.org/10.4049/JIMMUNOL.180.4.2376
Kwon YM, et al. Maternal antibodies by passive immunization with formalin inactivated respiratory syncytial virus confer protection without vaccine-enhanced disease. Antiviral Res. Apr. 2014;104(1):1–6. https://doi.org/10.1016/J.ANTIVIRAL.2014.01.008.
Delgado MF, et al. Lack of antibody affinity maturation due to poor Toll-like receptor stimulation leads to enhanced respiratory syncytial virus disease. Nat Med. Jan. 2009;15(1):34–41. https://doi.org/10.1038/NM.1894.
Domachowske JB et al. Sep., Safety, Tolerability and Pharmacokinetics of MEDI8897, an Extended Half-life Single-dose Respiratory Syncytial Virus Prefusion F-targeting Monoclonal Antibody Administered as a Single Dose to Healthy Preterm Infants, Pediatric Infectious Disease Journal, vol. 37, no. 9, pp. 886–892, 2018, https://doi.org/10.1097/INF.0000000000001916
Stewart L, Ryan KJ, Seare JG, Pinsky B, Becker L, Frogel M. Association of RSV-related hospitalization and non-compliance with Palivizumab among commercially insured infants: A retrospective claims analysis. BMC Infect Dis. Jul. 2013;13(1):1–11. https://doi.org/10.1186/1471-2334-13-334/FIGURES/4.
Van Den Berg JP, Westerbeek EAM, Berbers GAM, Van Gageldonk PGM, Van Der Klis FRM, Van Elburg RM. Transplacental transport of IgG antibodies specific for pertussis, diphtheria, tetanus, haemophilus influenzae type b, and neisseria meningitidis serogroup C is lower in preterm compared with term infants. Pediatr Infect Disease J. 2010;29(9):801–5. https://doi.org/10.1097/INF.0B013E3181DC4F77.
Obando-Pacheco P, et al. Respiratory syncytial virus seasonality: A global overview. J Infect Dis. Apr. 2018;217(9):1356–64. https://doi.org/10.1093/INFDIS/JIY056.
Domachowske JB et al. Sep., Safety, Tolerability and Pharmacokinetics of MEDI8897, an Extended Half-life Single-dose Respiratory Syncytial Virus Prefusion F-targeting Monoclonal Antibody Administered as a Single Dose to Healthy Preterm Infants, Pediatric Infectious Disease Journal, vol. 37, no. 9, pp. 886–892, 2018, https://doi.org/10.1097/INF.0000000000001916
Zhu Q, et al. A highly potent extended half-life antibody as a potential Rsv vaccine surrogate for all infants. Sci Transl Med. May 2017;9.
Polack P. Respiratory syncytial virus during pregnancy. Clin Infect Dis. May 2018;66(11):1666–7. https://doi.org/10.1093/CID/CIX1091.
Drysdale SB et al. Dec., Nirsevimab for Prevention of Hospitalizations Due to RSV in Infants, N Engl J Med, vol. 389, no. 26, pp. 2425–2435, 2023, https://doi.org/10.1056/NEJMOA2309189
Cber, Fda. Package Insert - ABRYSVO, Accessed: Jan. 10, 2025. [Online]. Available: http://vaers.hhs.gov
Walsh EE et al. Apr., A Randomized Phase 1/2 Study of a Respiratory Syncytial Virus Prefusion F Vaccine, J Infect Dis, vol. 225, no. 8, pp. 1357–1366, 2022, https://doi.org/10.1093/INFDIS/JIAB612
Falsey R, et al. Phase 1/2 randomized study of the Immunogenicity, Safety, and tolerability of a respiratory syncytial virus prefusion F vaccine in adults with concomitant inactivated influenza vaccine. J Infect Dis. Jun. 2022;225(12):2056–66. https://doi.org/10.1093/INFDIS/JIAB611.
Peterson JT, et al. Safety and immunogenicity of a respiratory syncytial virus prefusion F vaccine when coadministered with a Tetanus, Diphtheria, and acellular pertussis vaccine. J Infect Dis. Jun. 2022;225(12):2077–86. https://doi.org/10.1093/INFDIS/JIAB505.
Simões EAF, et al. Prefusion F Protein–Based respiratory syncytial virus immunization in pregnancy. N Engl J Med. Apr. 2022;386(17):1615–26.
Schmoele-Thoma B et al. Jun., Vaccine Efficacy in Adults in a Respiratory Syncytial Virus Challenge Study, N Engl J Med, vol. 386, no. 25, pp. 2377–2386, 2022, https://doi.org/10.1056/NEJMOA2116154
Baker J, et al. Equivalent immunogenicity across three RSVpreF vaccine lots in healthy adults 18–49 years of age: results of a randomized phase 3 study. Vaccine. May 2024;42:3172–9. https://doi.org/10.1016/J.VACCINE.2024.03.070.
Papazisis, Topalidou X, Maternal Vaccination for the Prevention of Infantile RSV Disease: An Overview of the Authorized, In-Progress, and, Vaccine R, Candidates A. 2024, https://doi.org/10.3390/VACCINES12090980/S1
Study Details | A Study to Learn About the Vaccine RSVpreF. In Pregnant Participants With HIV and Their Infants | ClinicalTrials.gov. Accessed: Jan. 13, 2025. [Online]. Available: https://clinicaltrials.gov/study/NCT06325657
Schwarz TF et al. Jun., Three Dose Levels of a Maternal Respiratory Syncytial Virus Vaccine Candidate Are Well Tolerated and Immunogenic in a Randomized Trial in Nonpregnant Women, J Infect Dis, vol. 225, no. 12, pp. 2067–2076, 2022, https://doi.org/10.1093/INFDIS/JIAB317
Bebia Z et al. Aug., Safety and Immunogenicity of an Investigational Respiratory Syncytial Virus Vaccine (RSVPreF3) in Mothers and Their Infants: A Phase 2 Randomized Trial, J Infect Dis, vol. 228, no. 3, pp. 299–310, 2023, https://doi.org/10.1093/INFDIS/JIAD024
Hermida N, et al. Safety and immunogenicity of respiratory syncytial virus prefusion maternal vaccine coadministered with Diphtheria-Tetanus-Pertussis vaccine: A phase 2 study. J Infect Dis. Aug. 2024;230(2):e353–62. https://doi.org/10.1093/INFDIS/JIAD560.
Dieussaert et al. Mar., RSV Prefusion F Protein–Based Maternal Vaccine — Preterm Birth and Other Outcomes, New England Journal of Medicine, vol. 390, no. 11, pp. 1009–1021, 2024,
GSK -. A study of safety, reactogenicity and immune response of the repeat vaccination against RSV when given to female participants of 18–49 years of age during their subsequent uncomplicated pregnancy. Accessed: Jan. 13, 2025. [Online]. Available: https://www.gsk-studyregister.com/en/trial-details/?id=214753
Bebia Z et al. Aug., Safety and Immunogenicity of an Investigational Respiratory Syncytial Virus Vaccine (RSVPreF3) in Mothers and Their Infants: A Phase 2 Randomized Trial, J Infect Dis, vol. 228, no. 3, pp. 299–310, 2023, https://doi.org/10.1093/INFDIS/JIAD024
GSK -. A follow-up study to describe the safety of study participants who received RSVPreF3 maternal vaccination (any dose) or controls from previous RSV MAT studies during any pregnancy conceived post vaccination/control. Accessed: Jan. 13, 2025. [Online]. Available: https://www.gsk-studyregister.com/en/trial-details/?id=219510
Chime N, et al. Phase 3 study assessing Lot-to-lot consistency of RSVPreF3 vaccine and its immune Response, Safety, and reactogenicity when Co-administered with FLU-D-QIV. J Infect Dis Jul. 2024. https://doi.org/10.1093/INFDIS/JIAE342.
Study Results. | A Study to Evaluate the Safety and Immune Response to an Unadjuvanted RSV Maternal Vaccine in Healthy Non-pregnant Females From 9 to 49 Years of Age | ClinicalTrials.gov. Accessed: Jan. 13, 2025. [Online]. Available: https://clinicaltrials.gov/study/NCT05169905?tab=results
Schwarz TF et al. Oct., Immunogenicity and Safety of 3 Formulations of a Respiratory Syncytial Virus Candidate Vaccine in Nonpregnant Women: A Phase 2, Randomized Trial, Journal of Infectious Diseases, vol. 220, no. 11, pp. 1816–1825, 2019, https://doi.org/10.1093/INFDIS/JIZ395
Glenn M, et al. Safety and immunogenicity of a Sf9 insect cell-derived respiratory syncytial virus fusion protein nanoparticle vaccine. Vaccine. Jan. 2013;31(3):524–32. https://doi.org/10.1016/J.VACCINE.2012.11.009.
Glenn GM, Randomized A, et al. Blinded, Controlled, Dose-Ranging study of a respiratory syncytial virus Recombinant fusion (F) nanoparticle vaccine in healthy women of childbearing age. J Infect Dis. Feb. 2016;213(3):411–22. https://doi.org/10.1093/INFDIS/JIV406.
August, et al. A phase 2 randomized, observer-blind, placebo-controlled, dose-ranging trial of aluminum-adjuvanted respiratory syncytial virus F particle vaccine formulations in healthy women of childbearing age. Vaccine. Jun. 2017;35:3749–59. https://doi.org/10.1016/J.VACCINE.2017.05.045.
Muňoz FM et al. Oct., Safety and Immunogenicity of a Respiratory Syncytial Virus Fusion (F) Protein Nanoparticle Vaccine in Healthy Third-Trimester Pregnant Women and Their Infants, J Infect Dis, vol. 220, no. 11, pp. 1802–1815, 2019, https://doi.org/10.1093/INFDIS/JIZ390
RSV Vaccine in Pregnancy - Health Research Authority. Accessed: Jan. 13, 2025. [Online]. Available: https://www.hra.nhs.uk/planning-and-improving-research/application-summaries/research-summaries/rsv-vaccine-in-pregnancy/
Shaw CA, et al. Safety and immunogenicity of an mRNA-Based RSV vaccine including a 12-Month booster in a phase 1 clinical trial in healthy older adults. J Infect Dis. Sep. 2024;230(3):e647–56. https://doi.org/10.1093/INFDIS/JIAE081.
A Study of mRNA-1345. Vaccine Targeting Respiratory Syncytial Virus in Pregnant Women and in Infants Born to Vaccinated Mothers | Clinical Research Trial Listing. Accessed: Jan. 13, 2025. [Online]. Available: https://www.centerwatch.com/clinical-trials/listings/NCT06143046/a-study-of-mrna-1345-vaccine-targeting-respiratory-syncytial-virus-in-pregnant-women-and-in-infants-born-to-vaccinated-mothers
Leroux-Roels et al. Feb., Double-Blind, Placebo-Controlled, Dose-Escalating Study Evaluating the Safety and Immunogenicity of an Epitope-Specific Chemically Defined Nanoparticle RSV Vaccine, Vaccines (Basel), vol. 11, no. 2, 2023, https://doi.org/10.3390/VACCINES11020367
Willemsen E, Borghans JAM, Bont LJ, Drylewicz J. Maternal vaccination against RSV can substantially reduce childhood mortality in low-income and middle-income countries: A mathematical modeling study, Vaccine X, vol. 15, p. 100379, Dec. 2023, https://doi.org/10.1016/J.JVACX.2023.100379
Scheltema NM, et al. Global respiratory syncytial virus-associated mortality in young children (RSV GOLD): a retrospective case series. Lancet Glob Health. Oct. 2017;5(10):e984–91. https://doi.org/10.1016/S2214-109X(17)30344-3.
06a-Annex C. Respiratory Syncytial Virus Investment Case Vaccine Investment Strategy Programme and Policy Committee Meeting, Accessed: Jan. 14, 2025. [Online]. Available: www.gavi.org.
Vaccine Investment Strategy. 2024. Accessed: Jan. 14, 2025. [Online]. Available: https://www.gavi.org/our-alliance/strategy/vaccine-investment-strategy-2024
Brand SPC, Munywoki P, Walumbe D, Keeling MJ, Nokes DJ. Reducing RSV hospitalisation in a lower-income country by vaccinating mothers-to-be and their households. Elife. Mar. 2020;9. https://doi.org/10.7554/ELIFE.47003.
Poletti P, et al. Evaluating vaccination strategies for reducing infant respiratory syncytial virus infection in low-income settings. BMC Med. Mar. 2015;13(1):1–11. https://doi.org/10.1186/S12916-015-0283-X/FIGURES/4.
Rainisch G, Adhikari B, Meltzer MI, Langley G. Estimating the impact of multiple immunization products on medically-attended respiratory syncytial virus (RSV) infections in infants. Vaccine. Jan. 2020;38(2):251–7. https://doi.org/10.1016/J.VACCINE.2019.10.023.
A Roadmap for Advancing RSV Maternal Immunization | PATH. Accessed: Jan. 14, 2025. [Online]. Available: https://www.path.org/our-impact/resources/roadmap-advancing-rsv-maternal-immunization/
Krishnaswamy S, Lambach P, Giles ML. Key considerations for successful implementation of maternal immunization programs in low and middle income countries. Hum Vaccin Immunother. Apr. 2019;15(4):942–50. https://doi.org/10.1080/21645515.2018.1564433.
Giles ML et al. Jul., Antenatal care service delivery and factors affecting effective tetanus vaccine coverage in low- and middle-income countries: Results of the Maternal Immunisation and Antenatal Care Situational analysis (MIACSA) project, Vaccine, vol. 38, no. 33, pp. 5278–5285, 2020, https://doi.org/10.1016/J.Vaccine.2020.05.025
Giles ML et al. Jul., Vaccine implementation factors affecting maternal tetanus immunization in low- and middle-income countries: Results of the Maternal Immunization and Antenatal Care Situational Analysis (MIACSA) project, Vaccine, vol. 38, no. 33, pp. 5268–5277, 2020, https://doi.org/10.1016/J.Vaccine.2020.05.084
Payne AB, Battan-Wraith S, Rowley EAK, Stockwell MS, Tartof SY, Dascomb K, Irving SA, Dixon B, Ball SW, Tenforde MW, Vazquez-Benitez G, Stephens AB, Han J, Natarajan K, Salas SB, Bezi C, SY LS, Lewin B, Sheffield T, Arndorfer J, Bride D, van Otterloo J, Naleway AL, Koppolu PD, Grannis S, Fadel W, Rogerson C, Duszynski T, Reese SE, Mitchell PK, Chickery S, Moline HL, Najdowski M, Ciesla AA, Reeves EL, Desilva M, Fleming-Dutra KE, Link-Gelles R. Effectiveness of nirsevimab among infants in their first RSV season in the united States, October 2023-March 2024: a test-negative design analysis. Lancet Reg Health Am. 2025;49:101196.
Phillips B, Jackson C, Phillips J. 2025. Clesrovimab for the prevention of respiratory syncytial virus lower respiratory tract disease in infants. J Pharm Technol, 87551225251392119.
Funding
Not Applicable.
Author information
Authors and Affiliations
Contributions
RA, RD, MKS, JH-B, JS-R, DC made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas that is revising or critically reviewing the article; giving final approval of the version to be published; agreeing on the journal to which the article has been submitted; and confirming to be accountable for all aspects of the work. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not Applicable.
Consent for publication
Not Applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

{kind=link}
Cite this article
Amin, R., Darwin, R., Sarma, M.K. et al. Maternal RSV immunization: clinical efficacy, immunological mechanisms and public health implications for preventing infant lower respiratory tract infection. J Health Popul Nutr 45, 105 (2026). https://doi.org/10.1186/s41043-026-01270-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1186/s41043-026-01270-5